Introduction: A Window That Never Opens Twice
There exists a period in human life during which every nutritional decision every food consumed, every feeding practice adopted, every harmful exposure avoided leaves a lasting biological imprint upon a developing organism. This period is known scientifically as the first 1,000 days: the interval stretching from conception to a child’s second birthday. During this critical window, the microbial colonisation of the body and the simultaneous maturation of the immune system reach their peak plasticity, thereby establishing the foundations of long-term health.
What was for decades regarded as a passive process the simple colonisation of the intestine by environmental bacteria has been fundamentally redefined by the scientific evidence accumulated in recent years. We now know that the gut microbiome does not merely accompany development: it actively directs it. It programmes immune tolerance, structures the intestinal barrier, regulates energy metabolism, modulates the gut-brain axis, and largely determines an individual’s vulnerability or resilience to a broad spectrum of chronic diseases. At the centre of this entire biological architecture lies a factor that is modifiable, accessible, and of enormous therapeutic potential: nutrition.
The Starting Point: The Mother as the First Microbial Environment
The programming of the infant microbiome does not begin at the moment of birth. It begins before. Maternal metabolic health and dietary intake during pregnancy largely determine the wellbeing of the developing foetus, given that the maternal gut microbiome generates metabolites which, present at critical moments of foetal development, actively participate in the epigenetic programming of the nascent organism.
Three metabolite groups merit particular clinical attention: short-chain fatty acids (SCFAs), produced through bacterial fermentation of dietary fibre; ligands of the aryl hydrocarbon receptor (AhR), responsive to dietary and microbial compounds; and vitamin A derivatives, implicated in the development of secondary lymphoid organs during embryogenesis. These compounds function as molecular signals capable of participating in foetal programming events at very precise embryological moments.
Maternal diet during gestation is not, therefore, simply a source of nutrients for foetal growth. It is the first regulator of the microbial ecosystem the infant will inherit. A maternal diet based on fibre-rich foods and fermented products supports a beneficial, diverse gut microbiota, whereas diets high in saturated fats and refined sugars the Western dietary pattern can promote states of dysbiosis with metabolic and immunological consequences that are transmitted to the offspring. Research has demonstrated that maternal exposure to a high-fat diet during pregnancy leaves a lasting metabolic imprint upon the neonatal innate immune system, altering the inflammatory state of the offspring’s microbiota and predisposing the individual to obesity and metabolic diseases in later life.
Furthermore, maternal dysbiosis during gestation has been linked to obstetric complications such as gestational diabetes, pre-eclampsia, and preterm birth all conditions which, in turn, compromise the initial microbial colonisation of the newborn. The causal chain is clear: maternal diet shapes the maternal microbiota, which in turn conditions gestational health, which ultimately determines the infant’s microbial starting point.
Birth: The First Major Nutritional-Microbial Event
The moment of birth represents the first large-scale transfer of microorganisms from mother to child. In a vaginal delivery, the newborn is exposed to the maternal vaginal and faecal microbiota rich in Lactobacillus, Bifidobacterium, and other key species which initiates the process of intestinal colonisation. In a caesarean delivery, this exposure is replaced by cutaneous and environmental microorganisms, generating a significantly different microbial profile, with lower abundance of Bifidobacterium and greater presence of potentially pathogenic species.
Gestational age at birth, mode of delivery, neonatal feeding practices, and exposure to perinatal antibiotics are primary determinants of the composition of the infant gut microbiome, and the resulting dysbiosis can alter developmental programming with adverse long-term health consequences. This microbial starting point is not neutral: it conditions the speed and quality of immune maturation, the integrity of the intestinal barrier, and the organism’s capacity to tolerate dietary and environmental antigens.
Breastfeeding: The Food That Also Nourishes the Microbiome
If there is a single nutritional factor with the greatest documented impact on the composition of the infant microbiome, it is breastfeeding. In the complex process of intestinal microbial assembly during the first months of life, breastfeeding is considered one of the most significant drivers of infant gut microbiota development, with lasting implications for health.
The central mechanism of this effect lies in human milk oligosaccharides (HMOs) a family of complex carbohydrates that the infant cannot digest directly but which act as selective substrates for specific intestinal bacteria. HMOs selectively promote the colonisation of Bifidobacterium species, which during the first months of life may represent between 50 and 70 per cent of the entire infant intestinal microbiota. This dominance of Bifidobacterium is not a minor detail: these bacteria produce acetate, formate, and lactate precursors which other microbial species convert into SCFAs metabolise tryptophan into indole-3-lactic acid (ILA), a potent anti-inflammatory compound that interferes with the transcription of the pro-inflammatory cytokine IL-8 in enterocytes, and compete actively with potentially pathogenic microorganisms for resources and intestinal niche space.
Higher levels of HMOs and SCFAs derived from sustained breastfeeding are associated with reduced risk of allergic disease, improved cognitive development, and lower incidence of obesity and diabetes in later life. The difference between a breastfed infant and one fed with formula is not exclusively nutritional in the classical sense: it is fundamentally microbial and immunological.
Differences in intestinal microbial communities between breastfed and formula-fed infants have been consistently observed in the scientific literature, and it is hypothesised that these differences partially mediate the relationship between breastfeeding and reduced risk of numerous communicable and non-communicable diseases during early childhood.

SCFAs: The Molecular Language Between Diet and the Immune System
Short-chain fatty acids principally butyrate, propionate, and acetate are the most widely studied metabolites in the diet-microbiota-immune system interaction. They are produced through bacterial fermentation of non-digestible dietary fibre and constitute the primary energy source of colonocytes, whilst simultaneously regulating intestinal permeability, the inflammatory response, and immune cell differentiation.
Maternal diet influences faecal bacterial composition, particularly through microbiota-accessible carbohydrates (MACs), which select SCFA-producing bacteria. There is compelling evidence that variations in maternal intake of these carbohydrates, intestinal bacterial composition, and SCFA production during gestation influence the development of the foetal immune system.
The deficit of SCFAs represents one of the most clinically relevant mechanisms connecting early dysbiosis with subsequent disease development. Without sufficient circulating butyrate, colonocytes lack the energy substrate required to maintain intestinal barrier integrity. Without adequate propionate, glucose regulation and satiety mechanisms are compromised. Without sufficient acetate, the activation of regulatory T cells is limited and immune tolerance weakens. The result is a permeable intestine, a dysregulated inflammatory response, and an immune system that fails to learn to distinguish adequately between self and non-self.
Complementary Feeding: The Second Major Nutritional Opportunity
The complementary feeding period, spanning from 6 to 24 months of age, marks the transition from an exclusively liquid diet to a dietary pattern incorporating solid foods to meet the infant’s growing nutritional demands. This process coincides with other critical developmental windows, including the maturation of the gut microbiome.
The bacterial family Bifidobacteriaceae predominates during the first six months of life, but following the introduction of solid foods, a progressive shift towards Lachnospiraceae, Ruminococcaceae, and Clostridium species is observed, reflecting the expansion of the intestinal ecosystem’s fermentative capacities in response to new dietary substrates. This shift in microbial architecture is not incidental: it represents the functional maturation of the microbiome towards an adult profile, with greater capacity for fibre fermentation, SCFA production, and immune modulation.
Dietary diversification through fibre- and protein-rich foods exerts particularly potent effects upon microbial diversity and interspecies interactions, facilitating the cooperative breakdown of resistant starches and plant polysaccharides. Conversely, diets of limited variety, poor in fibre and rich in refined sugars during this period perpetuate microbial immaturity and immunological vulnerability. Dietary diversity during complementary feeding is, in terms of microbial health, as important as breastfeeding was in the preceding months.
Nutrients play a crucial role in enriching and diversifying the microbiota, not only through solid foods but also through maternal dietary patterns during gestation, whose influence projects onto the microbial composition of the child.
The Consequences of Early Dysbiosis: Diseases That Begin in the Gut
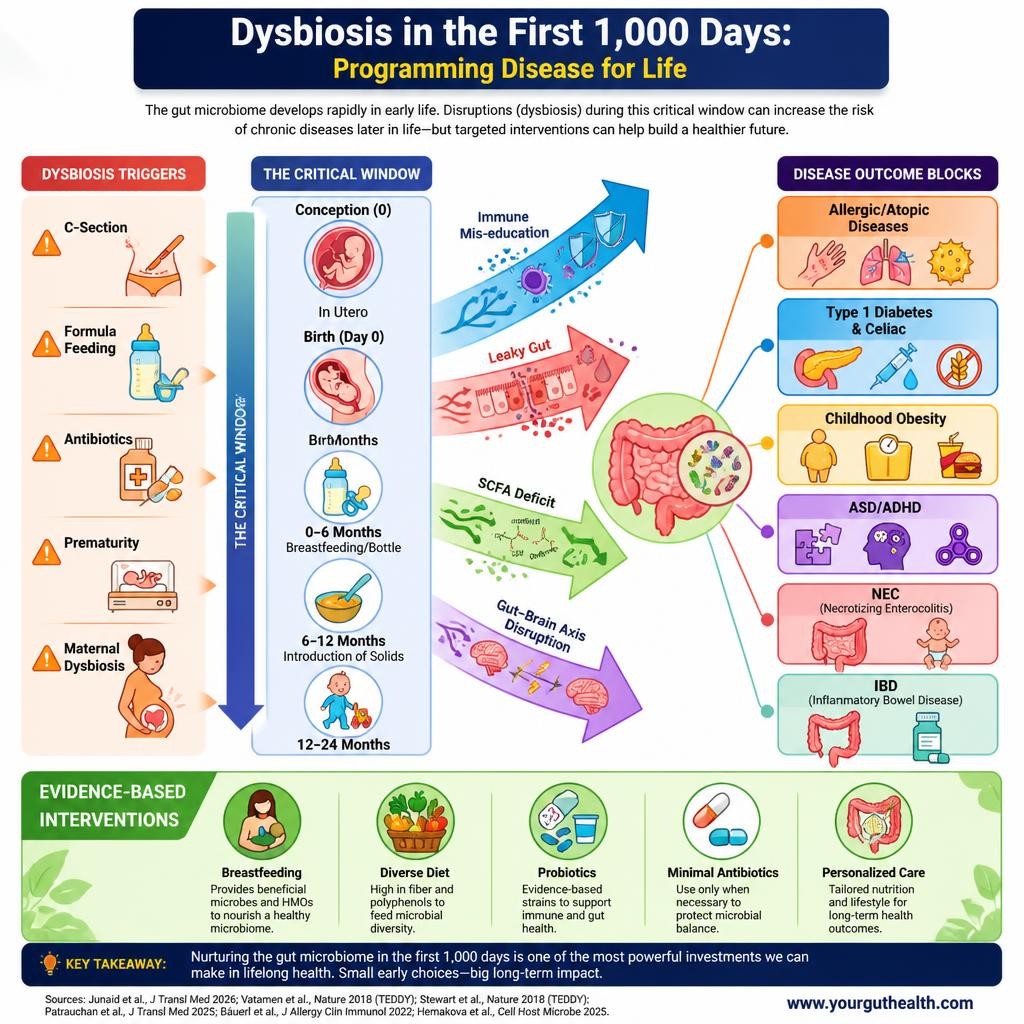
When the microbiome of the first 1,000 days develops under suboptimal conditions due to caesarean delivery, antibiotic use, absence of breastfeeding, poor-quality maternal or infant nutrition, prematurity, or pre-existing maternal dysbiosis the consequences are not limited to the neonatal period. Non-communicable diseases, with phenotypes ranging from chronic immuno-inflammatory conditions to neuropsychiatric disorders, have their roots in the earliest stages of life, and a growing number are linked to alterations in the composition and function of the gut microbiome.
The principal pathogenic mechanisms of dysbiosis include impairment of the intestinal mucosal barrier function, reduction in microbial diversity, decrease in beneficial microorganisms, and increase in potentially harmful species. This scenario has been associated with elevated risk of allergic and atopic diseases, Type 1 diabetes, coeliac disease, childhood obesity, autism spectrum disorder, ADHD, necrotising enterocolitis, and inflammatory bowel disease precisely the spectrum of conditions illustrated in the infographic upon which this article is based.
Emerging evidence suggests that alterations in the gut microbiota may play a significant role in the development of Type 1 diabetes during childhood, when the immune and metabolic systems are still in the process of maturation.
Interventions: What Nutrition Can Do
In the face of this landscape, the good news is that the mechanisms of microbial programming are, to a large extent, modifiable. The first 1,000 days offer a window of opportunity for interventions aimed at improving the child’s long-term health, and evidence from clinical trials demonstrates a wide range of potential targets for microbiota modulation during this continuum.
The interventions with the strongest scientific support are:
1. Optimisation of maternal diet during pregnancy: prioritising the consumption of fibre, fermented foods, omega-3 fatty acids, and key micronutrients such as folate, iron, and vitamin D all linked to a more diverse and balanced maternal microbiota.
2. Exclusive breastfeeding for the first six months of life: no infant formula is capable of replicating the bioactive complexity of human milk or its impact upon the infant microbiota.
3. Early and high-quality dietary diversification: introduction of varied foods rich in plant fibre, legumes, and quality proteins from six months of age, whilst avoiding ultra-processed dietary patterns from the outset.
4. Rational use of antibiotics: reserving their prescription for strict clinical indications, given the well-documented impact of antibiotics — particularly in the first years of life upon the diversity and stability of the microbiome.
5. Targeted probiotics and prebiotics: in situations of documented risk (caesarean delivery, prematurity, absence of breastfeeding), supplementation with specific strains such as Lactobacillus rhamnosus GG or Bifidobacterium longum subsp. infantis may contribute to restoring a more favourable microbial profile. Infants supplemented with probiotics during breastfeeding have shown higher counts of Bifidobacterium and Lactobacillus, as well as greater production of IgM, IgA, and IgG immunoglobulins at 12 months, compared with the placebo group.
Conclusion: To Nourish Is to Programme
The first 1,000 days are not simply a phase of growth. They are the period in which nutrition acts as an epigenetic language, as an immunological signal, as a microbial substrate, and as a metabolic code. Every dietary choice during this time by the mother before and during pregnancy, and by the infant during breastfeeding and complementary feeding writes instructions that the organism will read for decades to come.
The science confirms this with ever-increasing rigour: from conception and throughout the first years of life, maternal diet, metabolic status, and environmental exposures shape the microbial colonisation and maturation of the offspring, and the composition and diversity of the infant microbiome influence immune, metabolic, and neurodevelopmental processes.
As healthcare professionals, we have a responsibility to convey this knowledge to families in a clear, precise, and actionable manner. As parents and carers, you hold in your hands one of the most powerful preventive tools available: what you choose to eat, and what you choose to feed your child.
Your child’s microbiome is being shaped right now. The question is not whether nutrition matters. The question is whether we are prepared to act accordingly.
Selected References (PubMed / Indexed Journals):
- Noles et al., Nutrients 2025; doi:10.3390/nu17050743
- Rezai et al., Arch Clin Infect Dis 2025; doi:10.5812/archcid-163648
- Davis et al., J Allergy Clin Immunol 2022; doi:10.1016/j.jaci.2022.07.014
- Barrientos et al., Am J Reprod Immunol 2024; doi:10.1111/aji.13802
- Biagioli et al., Nutrients 2024; doi:10.3390/nu16020272
- Peng et al., Arch Gynecol Obstet 2024; doi:10.1007/s00404-023-07305-0
- Shen et al., MedComm 2025; doi:10.1002/mco2.70168
- Xi et al., Front Microbiol 2024; doi:10.3389/fmicb.2024.1356462
